Salivary Gland Cancer
Featured Expert:

What is salivary gland cancer?
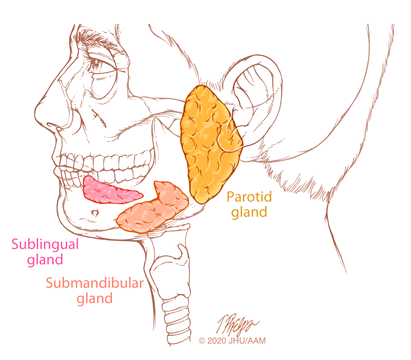
The salivary glands are comprised of both major and minor glands. The major glands are the bilateral parotid glands, submandibular glands and sublingual glands. The minor salivary glands are small glands distributed throughout the oral cavity, predominately on the palate, and in the upper aerodigestive tract.
Most salivary gland tumors are benign, and salivary gland cancers are uncommon malignancies that represent less than 5% of head and neck cancers. They are a heterogeneous group of tumors with varied clinical behavior. About 60% of malignant salivary gland tumors arise in the bilateral parotid glands, about 30% occur in the submandibular glands and 10%–15% originate in the sublingual and minor salivary glands.
What are the causes of salivary gland cancer?
Unlike other head and neck cancers that are caused by known carcinogens such as smoking and alcohol or HPV, the causes of most salivary gland cancers are often unclear. Radiation exposure, such as with prior low-dose therapeutic radiation therapy and multiple dental radiographs, is the most commonly suspected factor for the development of salivary gland neoplasms. Epstein Barr virus is associated with lymphoepithelial carcinoma. Other factors that have been implicated include workplace exposures (nickel, rubber, silica), diet, age and genetic susceptibility. In addition, pleomorphic adenoma can undergo malignant transformation in approximately 2% of cases.
Skin cancers such as squamous cell carcinoma and melanoma can metastasize to lymph nodes in and near the bilateral parotid glands, and thus mimic a primary parotid tumor.

Johns Hopkins Head and Neck Cancer Surgery Specialists
Our head and neck surgeons and speech language pathologists take a proactive approach to cancer treatment. Meet the Johns Hopkins specialists who will work closely with you during your journey.
What are the symptoms of salivary gland cancer?
Most salivary gland cancers arising in the bilateral parotid and submandibular glands present as a mass in the gland, not uncommonly painless.
- For parotid cancers: Pain, sensory loss or difficulty open the jaw can occur.
- Probable cancer: rapid recent tumor enlargement, facial nerve weakness, deep tumor fixation and enlargement of the neck lymph node.
- Submandibular cancers usually present as a painless neck mass. When there is pain, this can be confused with an inflammatory disorder. Less common signs of submandibular gland cancers include tumor fixation, skin invasion, lower facial paralysis and enlarged neck nodes.
- Sublingual gland cancers usually present as a mass in the floor of the mouth.
Minor salivary gland tumors usually present as a non-ulcerated, painless submucosal mass of the oral cavity, typically in the hard or soft palate. Symptoms of minor salivary gland tumors depend on tumor location, extent, tumor type, and whether the tumor is causing a mass effect or is invading local structures.
How are salivary gland cancers diagnosed?
A thorough history and physical examination is important for the diagnosis of salivary gland cancer. Symptoms are carefully sought, including mass progression, pain, sensory loss or trismus. In addition, symptoms including facial weakness, facial asymmetry, facial spasm or twitching, and eye symptoms are sought. The patient’s medical history is queried, including prior radiation exposure and history of skin or other malignancy.
A complete head and neck examination is performed. The salivary glands are inspected and palpated for tumor size, consistency, and mobility relative to adjacent tissues. The neck is examined for enlarged lymph nodes. The function of the facial nerve and other cranial nerves is assessed.
Fine needle aspiration (FNA) biopsy is an accurate way to confirm the clinical suspicion of a tumor for parotid and submandibular masses. Ultrasound guidance can be helpful to insure proper tumor sampling with FNA. Incisional or punch biopsies are useful for the diagnosis of minor salivary gland tumors.
Imaging studies, MRI in particular, are helpful to assess the extent of the primary tumor and the potential spread of the cancer along nerves or to neck lymph nodes. Chest radiographs, CT scan and positron emission tomography (PET)/CT scan can be helpful to assess for distant metastases.
What is the treatment of salivary gland cancer?
Management of salivary gland cancers is complex. Optimal treatment and follow-up requires a multidisciplinary team with the full range of specialists and support services with expertise in management of these neoplasms. Surgery is the primary treatment for salivary gland cancers, with complete surgical resection of the primary tumor as the goal. A comprehensive neck dissection is indicated for clinically detected metastases to the neck lymph nodes. Reconstructive surgery may be performed during the primary surgery, depending on what structures are resected to ensure complete removal of the cancer — for example, the facial nerve, skin, soft tissues and bone. This ensures the best cosmetic and functional results.
Adjuvant radiation therapy is indicated for select patients with advanced stage and high grade cancers. In select patients with minor salivary gland cancer, primary radiation therapy is sometimes recommended if surgical resection is considered to be too morbid. Long-term clinical follow-up is important for patients who need to be treated for salivary gland cancers, as salvage surgery is feasible for select patients. All decisions are made with a multidisciplinary team.

Johns Hopkins Head and Neck Cancer Surgery
Our team offers comprehensive treatments for cancers affecting the nasal passages, sinuses, the throat and nearby areas. Our head and neck surgeons work closely with medical and radiation oncologists, endocrinologists and other specialists to provide well-rounded care.